All about the skin around the eyes and “drooping” eyelids
04/04/2025

04/08/2023
Refractive errors are common eye conditions that affect the eye's ability to focus light correctly, which can lead to blurred or distorted vision. We will explore each of these errors, how they affect vision, and how they can be corrected.
It's important to clarify a common confusion between two related but distinct terms: visual acuity and the prescription (optical correction) of glasses.
Visual acuity is the measure of the ability to distinguish between two different points at a certain distance. There are several scales, and commonly (but inaccurately) it's referred to as a percentage of vision because a scale between 0 and 1 is used in our environment. It's measured with and without glasses, but the most useful measurement is with the best possible correction, as it gives us an idea of how the eye is functioning.
The prescription is the measurement of the optical "defects" of an eye, a formula from which glasses are constructed. It takes this form: 90° (axis of astigmatism) -1.25 (astigmatism power) +2.00 (spherical defect, in this case hyperopia). It can be written in various ways, the axis of astigmatism can be given as positive or negative, but myopia is always given as negative and hyperopia and presbyopia as positive.
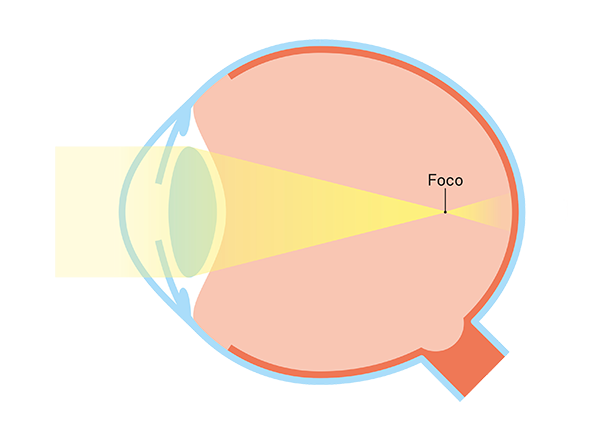
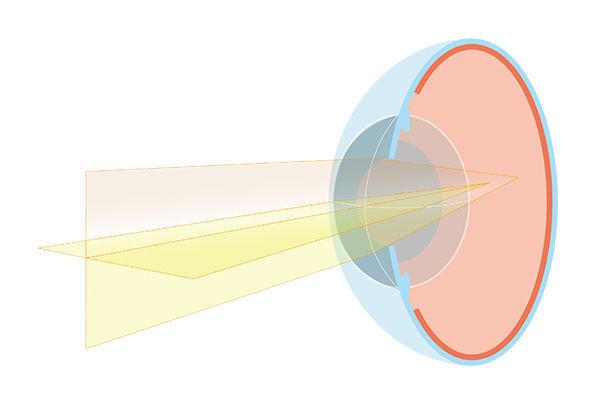
So, what factors determine if an eye needs a prescription to see well? What is seeing well? To see a clear image, light must focus on the plane of the retina with minimal dispersion, preferably on the macula and fovea (as it's the area with the highest concentration of receptors). What determines where the image focuses is the relationship between the eye's lens system and the distance between the corneal vertex and the fovea (known as axial length).
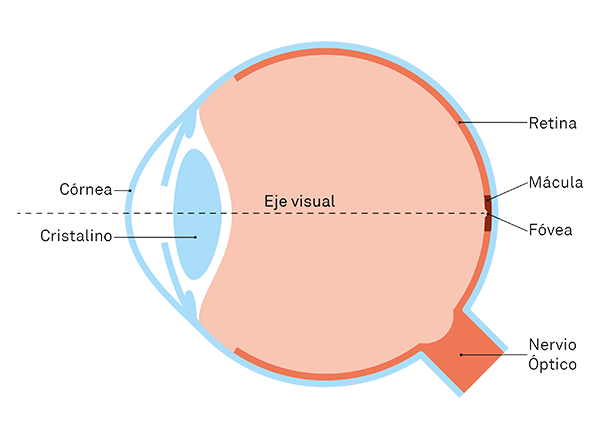
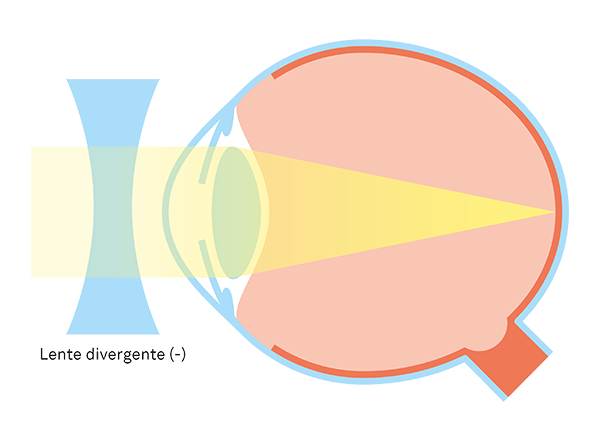
Regarding lenses, the most important ones are the cornea and the crystalline lens. Tears, aqueous humour, and vitreous humour also have an influence, but for practical purposes, it is minimal. If the eye is longer or the lenses are very powerful (relative to the relationship they have), the image is focused in front of the retina. We say that the eye is nearsighted (myopic).
To correct the focus, we use a divergent lens, which reduces the overall power. That's why, by convention, the negative sign is used for myopia.
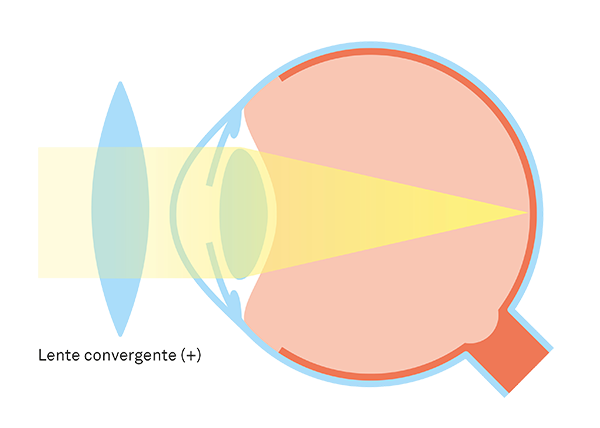
In the opposite case, if the image is focused (theoretically) behind the retina because the eye is shorter or the lenses have less power, we talk about hypermetropia (hyperopia).

To correct hyperopia, we use convergent lenses, which add power to the system.
It's relevant to bear in mind that we are not taking into account the eye's accommodation process. We are considering light coming from beyond one or two meters of distance, which for the eye is akin to infinity under normal conditions. Sometimes the eye accommodates when it shouldn't, and this can result in hidden hyperopia (compensated by accommodation, which is why if there are only a few dioptres, glasses might not be necessary as long as it doesn't generate symptoms) or "false" myopia (like the kind that can typically arise after a period of intense focus, such as during exams, for instance). This can primarily lead to headaches due to the strain and can only be diagnosed by an ophthalmologist, as it requires a test involving the use of eye drops known as cycloplegia.
From birth, we start to lose accommodation (the ability to focus on nearby objects, within less than 1 meter). However, it's around the age of 40-45 when it becomes significantly noticeable, as the capacity and the necessity for that effort become more balanced around that age. This is presbyopia or "tired eyes" (not to be confused with eye fatigue). What practically defines it is the need to switch between different prescriptions for near and far vision. It behaves like hyperopia, which is why the lens for presbyopia is also convergent (positive). For this reason, it's common for people with myopia to do without their glasses for close vision starting from that age.
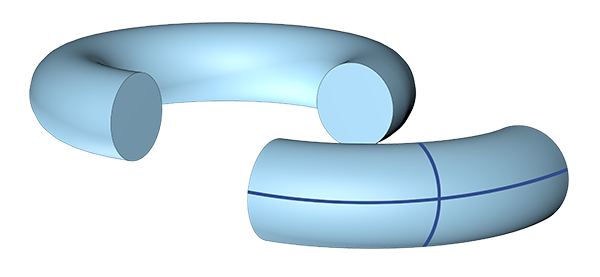
Astigmatism is a bit more complex, as we have to consider that the eye is a three-dimensional structure, not a flat lens. Essentially, it occurs when light rays are refracted differently depending on the point where they enter the eye.
This is the case because the eye is not a perfect sphere, and when it's "sufficiently flattened," the visual system behaves like a toroid. If we cut a section from the edge of a toroid or a "donut" and use it as a lens, we will observe that it doesn't refract light equally at all points. It will be more powerful along one axis and progressively less so as we rotate it by 90 degrees, perpendicular to the original axis.
For this reason, the prescription formula includes the axis of astigmatism: we are specifying what power needs to be applied at each point of the lens to compensate for the deviation. And we can use a positive or negative sign: we just need to indicate which axis we are referring to.
In conclusion, refractive errors like myopia, hyperopia, astigmatism, and presbyopia are common conditions that affect the eye's ability to focus light correctly. Fortunately, these refractive errors can generally be corrected using lenses such as glasses or contact lenses, which compensate for the optical irregularities of the eye and improve the quality of vision. It's important to undergo regular vision exams with an ophthalmologist to detect and correct any eye conditions or refractive errors, ensuring optimal vision at all distances.
Dr. Alberto Lozano, Ophthalmologist at the Barraquer Ophthalmology Centre
Almost all wearers of glasses and contact lenses consider reducing their prescription with refractive techniques at some point. In this chapter we explain all the options and help you know when it is worth having surgery, who is a good candidate and why it is so important to choose where to go.